Katelyn Dykstra Dykerman
On May 1, 2014, Dr Cary Gabriel Costello published a blog post entitled, “On Eugenic Abortion of the Intersex,” that discussed the contemporary choice for parents to terminate fetuses diagnosed with an intersex condition. His post provides a useful starting point for a discussion about the continued threat of eugenic science (or genetic science, under which eugenic practices have often been re-packaged) to queer folks, in particular those with intersex conditions.
A more comprehensive analysis of the issue Costello raises can be found in the September 2013 issue of The Journal of American Bioethics* which took up the practice of PGD (prenatal genetic diagnosis) in cases of intersex conditions. The focus article by Robert Sparrow explained that PGD can be used to “avoid the birth of an intersex child” (29). He explored the ethics of PGD for intersex conditions, hesitantly coming to the conclusion that, indeed, PGD is ethical in cases of intersex because people with intersex conditions are less likely to find community, sexual pleasure, and be able to reproduce. Thus, he places the responsibility on parents to consider whether they want to bring a child with genitals that may not be understood as “normal” into a hostile world. As responding authors pointed out, Sparrow’s analysis picks up eugenic rhetoric by asserting that there is a normal body to which all other bodies aspire. Any that do not fit into the ideal physical body, and resulting idealized life narrative, should be expunged — you know, for their own good. Ahem!
To be clear: Any medical decision that limits life based on specific social or cultural biases contains dangerous eugenic possibilities. I therefore think it useful to briefly return to the heyday of eugenic rhetoric in order to show how eugenic scientists discussed intersex conditions and thus demonstrate the ways in which Sparrow’s discourse picks it up and repackages it.
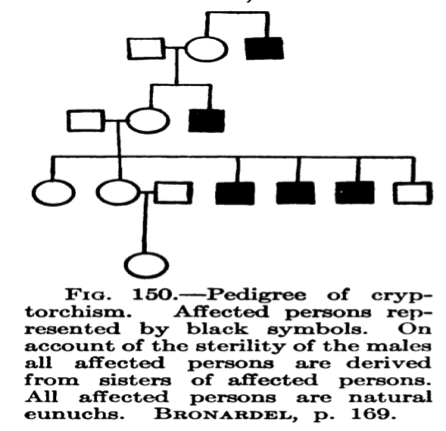
Eugenics, as a discourse, as well as a “pseudo-“science, encompasses both medicine and science and has thus been touted as a legitimate way of promoting — indeed, breeding — “normal bodies.” Despite the United States’ previously avid denials of its deep involvement in eugenic practices and research (see Edwin Black’s War Against the Weak), one of the most enthusiastic proponents for negative eugenics, Charles Davenport, was American. In 1911, Davenport published Heredity in Relation to Eugenics in which he took up the issue of “hermaphrodidic conditions,” which he genetically graphed (see example below). These graphs, called pedigrees, and his accompanying commentary, mark intersex conditions as both defective and abnormal. He claimed that an intersex condition occurs as a failure of “normal” development. He referred to hyperspadias conditions (one in which the opening to the urethra is not at the tip of the penis) as “imperfect,” thus marking the body with an intersex condition itself as not-perfect.
Moreover, the blame for the passing on of intersex conditions falls directly upon the mother, Davenport writes:
The eugenical conclusion is that females belonging to the hermaphrodidic (hypospadic or cryptorchitic [the absence of one or both testes]) strains, if married, will probably have at least half of their sons defective, particularly if they have defective brothers; but normal males of such strains may marry females from unaffected strains with impunity. (170)
What results from Davenport’s rhetoric here is two-fold. First, the condition itself is considered “defective” instead of simply a normal variation of the body. Second, this defect is carried in the woman’s genes, making the mother responsible for bestowing upon her child an unlivable life.
In eugenic rhetoric, the responsibility for the undesirable condition is always placed on the parent, in this case the maternal parent. In Sparrow’s more recent discussion, the decision about what to do (if anything) about the intersex condition firmly rests with the parents, leaving them responsible both for the condition as well as the life that follows from any decision they will make regarding it. The kind of eugenic rhetoric that would be familiar to Davenport has clearly not been expunged from the medical profession.
While there are some queer rights activists like Alice Domurat Dreger, Anne Fausto-Sterling, and Bo Laurent, closely associated with the medical establishment, who are working to erase this kind of harmful language and practice from its grey-green hallways, the exclusion of bodily difference is still firmly entrenched in popular medical language of “perfection” and “normalcy.” Jason Behrmann and Vardit Ravitsky point to this problem, claiming that the parents of intersex fetuses must take into account the social conditions into which they will bring their “offspring” (39). These conditions are, in their opinion, fraught with misunderstandings regarding the complex “intertwining” of “sex, gender and sexual orientation” (39). Many of the responses to Sparrow’s article seem to echo this concern. Regardless of parents’ intentions, their decision whether or not to bring an intersex fetus to term is loaded with all kinds of social, medical, and cultural baggage and biases. It is problematic then, that the medical profession wields both the authority to council, and the ability to undertake PGD in cases of intersex.
Diana Aurenque and Hans-Jörg Ehni rightly argue that medical professionals, whenever they act upon their loaded perception of “normal,” are doing a disservice to their patients (56). “Normal” does not exist. It is a fiction, a socially and culturally constructed fiction. I would argue that any unnecessary intervention (that is, one that does not work to save biological life) on the part of a medical profession to achieve “normal” is an act of eugenics. As the example of Davenport’s text illuminates, it is through language that we construct a “normal” body. The linguistic constructions of normal bodies then facilitate the very real acts of violent medical intervention that exclude intersex bodies from a livable life — or any life at all.
* Subsequent page numbers (excluding Davenport) refer to this edition of The Journal of American Bioethics.
 Katelyn Dykstra Dykerman is a PhD student at the University of Manitoba. Her research areas include intersex, bioethics, surgical ethics, and queer identity studies, within the vast scope of Modernist Literature. In her other life she is a mother and want-to-be gardener. She tweets from @katelynjane.
Katelyn Dykstra Dykerman is a PhD student at the University of Manitoba. Her research areas include intersex, bioethics, surgical ethics, and queer identity studies, within the vast scope of Modernist Literature. In her other life she is a mother and want-to-be gardener. She tweets from @katelynjane.

NOTCHES: (re)marks on the history of sexuality is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Based on a work at www.notchesblog.com.
For permission to publish any NOTCHES post in whole or in part please contact the editors at NotchesBlog@gmail.com





Intersex medical protocols are eugenic in principle, and in fact.
From the acceptance of abortion as a means of erasing intersex births, to the use of pre-natal dexamethasone to alter both behaviours and anatomies of targeted female children with CAH, to pre-natal genetic diagnosis that precludes the possibility of intersex births, it is quite evident that medicine regards intersex births as invalid human embodiment. Subsequent interventions in infancy and adolescence only reinforce that outlook.
Sparrow’s 2013 article received trenchant criticism from intersex advocates, both publicly and privately. I can vouchsafe for the fact that in attempting to address the points raised with him personally, it was quite apparent he was comfortable talking about intersex as a philosophical issue, and very uncomfortable talking to articulate intersex advocates.
I would also observe that Bo Laurent and Alice Dreger are two people very closely associated with the introduction of the term ‘DsD – Disorders of Sex Development’ as an umbrella description for anyone born intersex. Whilst clinicians have adopted the term wholesale, and parents often appear comfortable using the term, it is reviled by many people born intersex. Dr Anne Fausto-Sterling is highly regarded by many intersex advocates.
Leslie Jaye,
Thank you very much for these useful and considered insights. I definitely got the impression you describe from Sparrow’s article, which makes me wonder why they chose him to write it? Moreover, I wonder about your comment on the use of DSD (a term I am very uncomfortable with, and have rejected using in my work for the exact reason you describe), and the medical profession’s continued use of it in spite of being “reviled” by the community of intersex folks with lived experience. Do you see this denial as evidence of intersex conditions being hyper-medicalized in an effort to expunge embodied sexual difference? It also seems to me, and this might be an error on my part, that folks like Dreger have abandoned much of their work on intersex because the medical protocols used to “treat” intersex conditions are perhaps more subverted and covert — ie. not genital surgeries? Again, I might be misreading this, but it certainly is a trend I have noticed and has troubled me greatly. What do you think?
Georgiann Davis wrote an excellent critique about the adoption of the dsd terminology – ‘DSD is a Perfectly Fine Term’. I would recommend it. Professor Davis makes a very coherent case for dsd nomenclature contributing to the pathologising of intersex status.
The received wisdom that intersex is not a term that clinicians are comfortable with is not borne out by their own academic papers, you can also find it in the title of the Chicago Consensus Statement viz. ‘ Consensus Statement management of intersex disorders’. It is in their inter-actions with parents that clinicians with-hold the term; in much the same way as the various forms of hermaphrodite were in previous years. Clinicians are perfectly comfortable using the term between themselves.
Disorder is pejorative. So much so that clinicians strove mightily to drop it’s use in DSM5 when describing mental health issues. No such effort was made for intersex, although some clinicians are now using ‘differences’ or variations in a tacit admission that the terminology is not acceptable – even among some parents.
Ms Dreger’s close association with the adoption of dsd, and the reification of the medical model as the only means of addressing intersex has rather marked thier card. I will leave you to draw you own conclusions about that. You can find a lot of information about the duplicitous use of pre-natal dexamethasone @ fetaldex.org.
I am not at all sure where you gained the impression that genital surgeries are diminishing. Sarah Creighton and colleagues wrote a paper in 2013 that investigated this issue:-
“Childhood surgery for ambiguous genitalia: glimpses of practice changes or more of the same?”
In a detailed investigation of the current situation, they were moved to say, in conclusion:-
“Even with parental or adult consent, we would not consider requests for elective genital surgery without discussion and debate within a multidisciplinary team. On the whole there is much more discussion about any intervention.
On the other hand, we have also witnessed unabated enthusiasm for and confidence in childhood surgery.
To answer the question that is the title of this article from a purely surgical perspective, there is presently no definitive evidence that the consensus statement has had a significant impact on the number of children undergoing genital surgery. There is also, as yet, no new evidence for significant improvements in long-term post-operative outcomes.”
Pingback: Thoughts about the Future | Perceptions of Pregnancy
Pingback: ‘Paddy Petticoat’, a nineteenth-century Irish ‘hermaphrodite’ criminal. Part iii: The label | Elaine Farrell